
Prostate Cancer
Prostate cancer is the most common cancer in the male population, accounting for almost 23% of new tumors diagnosed in men. The risk of prostate cancer is linked to age, very few cases are diagnosed in men under 50 years of age and a large percentage of diagnoses occur in men over 70 years of age. Men with a family history of prostate cancer should begin screening at age 45.
In recent years there has been an increase in the detection of prostate cancer through the use of prostate specific antigen (PSA) blood tests and through surgery for benign prostate enlargement where material is sent for analysis to anatomic pathology and a diagnosis is made.
Diagnosis and staging
– Digital examination / digital rectal examination: consists of an examination in which the Urologist inserts a finger inside a lubricated glove into the rectum and palpates the prostate through the rectal wall in search of nodules or abnormal areas.
– Prostate-specific antigen (PSA): A laboratory test that measures PSA levels in the blood. This is a substance produced mostly by the prostate that is found in greater amounts in the blood of men who have prostate cancer. It is worth mentioning that the PSA result may also be elevated in men who suffer from an infection (Prostatitis) or inflammation of the prostate, or who have benign prostatic hyperplasia (BPH).
– Transrectal ultrasound: procedure in which a probe is inserted into the rectum to examine the prostate.
– Prostate biopsy: removal of cells or tissue for examination under a microscope. The pathologist examines the sample for cancer cells and determines the Gleason score. The Gleason score ranges from 2 to 10 and describes the biological activity and the likelihood of the tumor spreading. The lower the score, the lower the likelihood of tumor spread. Transrectal biopsy was the most traditional method and consists of the removal of prostate tissue by inserting a fine needle through the rectum into the prostate. This procedure is performed using transrectal ultrasound to guide the needle.
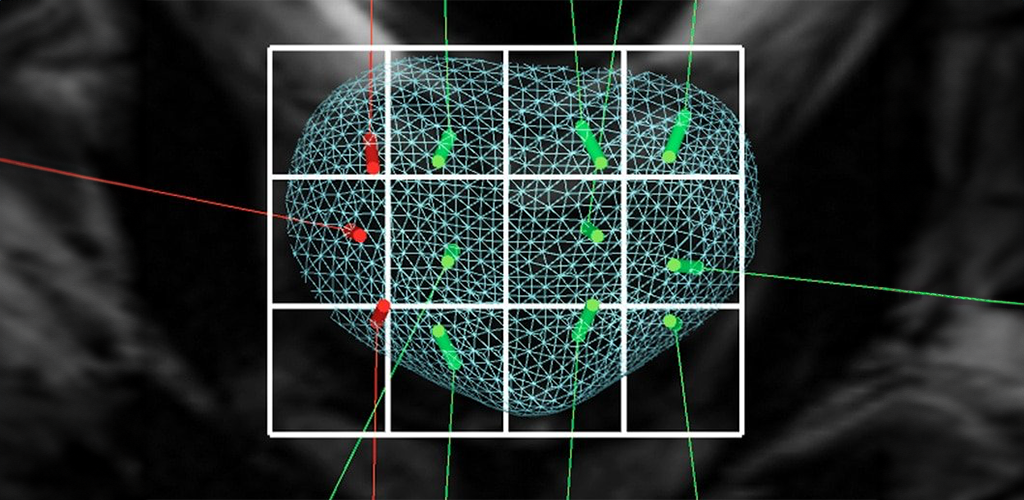
Multiparametric Magnetic Resonance Imaging and Fusion Biopsy
Changes in the diagnostic paradigm in prostate cancer.
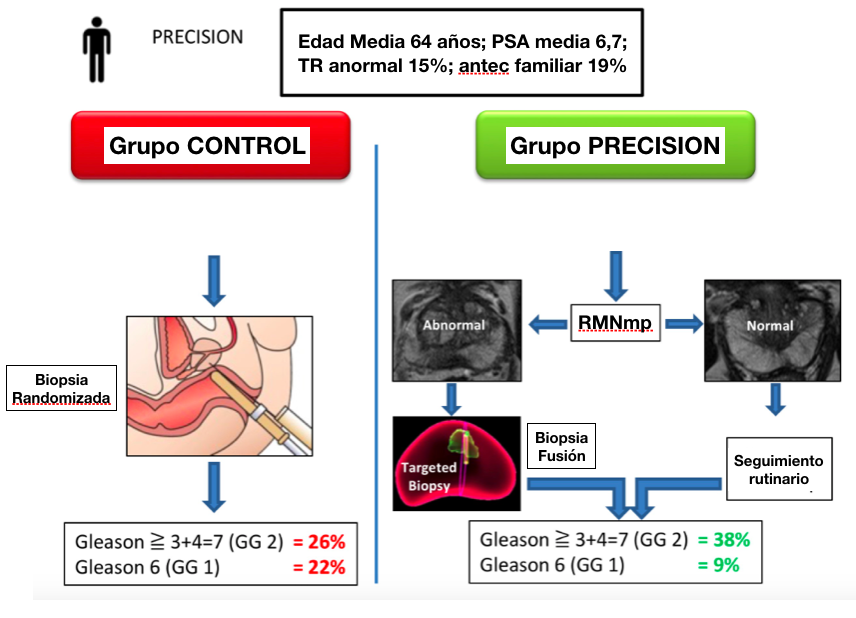
The recent study called PRECISION (Prostate Evaluation for Clinically Important disease: Sampling using Image-guidance Or Not?) published in the renowned journal The New England Journal of Medicine has shown results that impact the diagnosis of prostate cancer. In this international study, 500 men with suspected prostate cancer due to increased PSA (Prostate Specific Antigen) were separated into two groups.
In group 1, the traditional diagnostic method was performed using ultrasound-directed transrectal prostate biopsy and performing 12 biopsies, and in group 2, the diagnosis was made based on Multiparametric Magnetic Resonance Imaging (mpMRI) findings of the prostate. In the second group, if the MRI was abnormal, a prostate biopsy was performed by FUSION with software that integrates MRI and ultrasound images, performing only biopsies of the suspicious area of the MRI.
The primary objective sought in this study was the evaluation of the detection rate of clinically significant prostate cancer; and secondary objectives included the detection rate of clinically insignificant cancer (which is defined as organ-limited disease with a tumor volume <0.5 cm3, Gleason score 6, whose treatment is not necessary and will not benefit patients).
In Group 1 of traditional biopsy, the detection rate of clinically significant cancer was 26%, and the detection rate of clinically insignificant cancer was 22%. In Group 2 of the Resonance fusion, the clinically significant cancer detection rate of patients who will require treatment approximately doubled to 38% and the negligible cancer detection rate decreased to 9% by avoiding treating cancers that do not require treatment.
Thus, despite the fact that more than a quarter of the men in the MRI pathway actually avoided a biopsy, the detection rate of clinically significant prostate cancer was much higher in this arm. In addition, the detection rate of clinically insignificant cancer was much lower (i.e., overdiagnosis was reduced). And all this with only four biopsy takes, compared to 12 traditional biopsy takes with ultrasound.
These findings should prompt a change for patients in the diagnostic pathway for early prostate cancer in two ways:
1 All patients with a clinical suspicion of prostate cancer should be offered an MRI as part of their decision-making pathway prior to biopsy.
2 All patients with an abnormality on their MRI should be offered a fusion biopsy.
One cause for concern, are patients with a normal MRI (28% of patients), who despite clinical suspicion of prostate cancer, did not have a biopsy. How many clinically significant cancers could be missed by not offering a biopsy to those patients? One answer to what we would find is provided by the PROMIS (Prostate MR Imaging Study) which included an extensive biopsy for patients with a normal MRI.
Precise and permanent control of the images taken during the biopsies with fusion software. In those cases in which the MRI was normal (28% of individuals), no biopsy was performed and patients continued routine surveillance with PSA and digital rectal examination.
In the PROMIS study, the negative predictive value of MRI for detecting any type 4 cancer is 76%, i.e., up to 1 in 4 men will have pattern 4 cancer on transperineal biopsy. However, no primary cancers of pattern 4 were missed on MRI. The absence of some Gleason pattern 4 cancers in some men could be accepted, provided that “routine follow-up” is adequate.
This could provide sufficient evidence to fully embrace the indication of MRI in the approach to early detection of prostate cancer. Based on the PROMIS study, published in The Lancet 2017, added to the PRECISION study, the results provide the knowledge to fully integrate MRI in the evaluation of men with suspected prostate cancer. The era of randomized blind prostate biopsy is possibly over, except perhaps in those patients in whom MRI is contraindicated.
GENETIC MARKERS
► SelectMDx
The SelectMDx genetic marker helps to avoid unnecessary prostate biopsies. This study is performed in a urine test, it is a non-invasive study for the detection of the risk of aggressive prostate cancer.
► ConfirmMDx
The ConfirmMDX genetic marker for prostate cancer addresses the concerns of a false-negative prostate biopsy result.
The ConfirmMDX test for prostate cancer addresses the concerns of a false-negative biopsy and helps the urologist to:
– DISCARD men who do not have prostate cancer from undergoing unnecessary repeat biopsies.
– INCLUDE men at high risk who may need to be re-biopsied and undergo possible treatment.
DIAGNOSIS
Prognosis and treatment options depend on the following:
– The stage of the cancer (whether it affects part of the prostate, involves the entire gland, or has spread to other parts of the body).
– The patient’s age and general health.
– Whether the cancer has been newly diagnosed or has returned after being treated and apparently cured.
How is the Gleason grade established?
The pathologist assesses two areas or zones of the prostate tissue sample obtained by prostate biopsy. He tries to choose areas that are well representative of the tumor. Each of the two areas is assigned a score ranging from 1 to 5.
1 corresponds to cases of low aggressiveness of the tumor (clusters of cancer cells resemble normal prostate glands). From 2 to 4 include intermediate, progressively aggressive situations. To establish the Gleason grade of each case, the numbers assigned to each area are added together. For example: 3+ 4=7. Therefore, there is no Gleason O or 1, the minimum is 2 (1 + 1). The lower the Gleason, the lower the chance that the prostate cancer will be aggressive, grow more slowly and spread less. On the opposite side, the higher the Gleason, the greater the chance of tumor aggressiveness. In summary, Gleason scores between 2 and 4 correspond to low aggressiveness; 5 and 6 are intermediate situations and aggressiveness increases from 7 to 10.
Once prostate cancer has been diagnosed, tests will be performed to determine whether the cancerous cells have spread within the prostate or to other parts of the patient’s body. This process is called staging. It is necessary to know the stage of the disease in order to plan the most appropriate treatment.
To determine the stage of the prostate cancer it is usually indicated:
– Bone scintigraphy or radionuclide bone scan: A procedure to determine the presence of rapidly dividing cells in the bone, such as cancer cells.
– Computed tomography scan (CT scan) to evaluate the presence of affected nodes in the abdomen and pelvis.
– PET-PSMA Gallium: Procedure that adds the advantages of Computed Tomography to Nuclear Medicine, increasing the sensitivity and specificity of previous methods.
The stage of the cancer is based on the results of staging and diagnostic tests such as biopsy of the original tumor. The biopsy is used to determine the Gleason score.
Cancer spreads in the body in three ways:
– Through tissue. The cancer invades the surrounding normal tissue.
– Through the lymphatic system. Cancer invades the lymphatic system and circulates through the lymphatic vessels to other places in the body.
– Through the blood. Cancer invades the veins and capillaries and circulates through the blood to other places in the body.
When cancer cells break away from the primary (original) tumor and circulate through the lymph or blood to other places in the body, another (secondary) tumor may form. This process is called metastasis. The secondary (metastatic) tumor is the same type of cancer as the primary tumor. For example, if prostate cancer spreads to the bones, the cancer cells in the bones are actually prostate cancer cells. The disease is metastatic prostate cancer, not bone cancer.
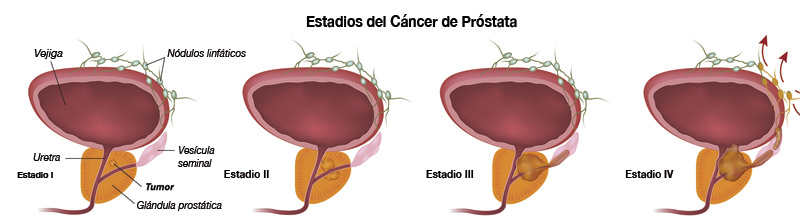
STAGES:
Stage I
The cancer is restricted to the prostate only. It cannot be felt during a digital rectal examination and is not visible by imaging. It is usually found incidentally during scheduled surgery for other reasons, such as benign prostatic hyperplasia. The Gleason score is low. Stage I prostate cancer may also be called stage A1 prostate cancer.
Stage II
The cancer is more advanced than stage I, but has not yet spread outside the prostate. The Gleason score can range from 2-10. Stage II prostate cancer may also be called stage A2, stage B1 or stage B2.
Stage III
Cancer has spread beyond the outer layer of the prostate to nearby tissues. Cancer may be found in the seminal vesicles. The Gleason score can range from 2-10. Stage III prostate cancer may also be called stage C prostate cancer.
Stage IV
The cancer has metastasized (spread) to lymph nodes near and not near the prostate to other parts of the body, such as the bladder, rectum, bones, or lungs. Prostate cancer often spreads to the bones. The Gleason score can range from 2-10. Stage IV prostate cancer may also be called stage D1 or D2 prostate cancer.
T1, T2, T3, T4
TREATMENTS
Patients in good health have usually been offered surgical treatment for prostate cancer, the most recommended being Radical Prostatectomy.
Laparoscopic Radical Prostatectomy This technique is performed through 5 small incisions in the abdomen.
Laparoscopic radical prostatectomy is an accepted and established treatment for localized prostate cancer.
This surgical technique is performed according to the principles of open surgery but without the surgeon’s hand entering the patient’s abdomen. The lenses of the laparoscope, connected to the camera, project to the monitor an excellent image magnifying the details of the prostate. Once the prostate is freed from the neighboring organs, it is placed in a plastic bag and extracted through one of the orifices created for the procedure. The bladder is “reattached” to the urethra to restore the continuity of the urinary tract using laparoscopic techniques.
The hospital stay is usually 3 to 5 days, where it is necessary to wear a bladder catheter for 7 days or more to empty the bladder and allow the urethra-bladder connection to heal properly.
Pelvic lymphadenectomy
Surgical procedure in which the pelvic lymph nodes are removed. The pathologist examines a tissue sample under a microscope to look for cancer cells. If the nodes contain cancer, the doctor does not remove the prostate and may recommend other treatment.
OPEN RADICAL PROSTATECTOMY
This surgical procedure has most often been used to remove the prostate, surrounding tissue and seminal vesicles. There are different types of open radical prostatectomy:
► Retropubic prostatectomy.
Surgical procedure to remove the prostate through a cut (incision) in the abdominal wall. Because radical prostatectomy is a radical surgical procedure, patients may need to receive blood transfusions. Patients are usually hospitalized for approximately 5 days. The bladder catheter remains in place for two to three weeks and full recovery may take up to 12 weeks.
► Common complications of open prostate surgery.
The most common complications when a patient must undergo conventional prostate surgery are: sexual impotence, urine incontinence, bleeding and post-operative. The most significant long-term adverse effect of conventional surgery is urinary incontinence, which is the inability to control urinary flow or the partial ability to hold back the urinary stream usually characterized by urine leakage on coughing or straining requiring the use of protective drapes.
► Perineal prostatectomy.
Surgical procedure by which the prostate is removed through an incision (cut) made in the perineum (area between the scrotum and anus). The lymph nodes may also be removed through another incision in the abdomen.
In addition, the following types of surgical interventions are practiced:
► Laparoscopic Radical Prostatectomy.
This technique is performed through 5 small incisions in the abdomen. Laparoscopic radical prostatectomy is an accepted and established treatment for localized prostate cancer.
This surgical technique is performed according to the principles of open surgery but without the surgeon’s hand entering the patient’s abdomen. The lenses of the laparoscope, connected to the camera, project to the monitor an excellent image magnifying the details of the prostate. Once the prostate is freed from the neighboring organs, it is placed in a plastic bag and extracted through one of the orifices created for the procedure. The bladder is “reattached” to the urethra to restore the continuity of the urinary tract using laparoscopic techniques.
The length of hospitalization is usually 3 to 5 days, during which it is necessary to wear a bladder catheter for 10 days or more to empty the bladder and allow proper healing of the urethra-bladder connection.
► Pelvic lymphadenectomy.
Surgical procedure in which lymph nodes are removed from the pelvis. The pathologist examines a tissue sample under a microscope to look for cancer cells. If the nodes contain cancer, the doctor may recommend other treatment.
Da Vinci Xi Robotic Prostatectomy
The da Vinci Surgical System provides surgeons with an alternative to both traditional open surgery and conventional laparoscopy by placing the surgeon’s hands at the controls of a state-of-the-art robotic platform. The da Vinci Xi Robot enables surgeons to perform even the most complex and delicate procedures through very small incisions with unprecedented precision, improving surgeon dexterity and optimizing outcomes.
It translates the surgeon’s movements intuitively, allowing full control of the fiber optics and instruments, avoiding complex laparoscopic movements;
It allows a real three-dimensional view of the operating field: the surgeon literally enters into a process of “immersion”, in order to best assess the anatomical dissection planes and “live” the surgical intervention almost from inside the patient’s body.
For prostate cancer, he incorporates the best techniques of traditional surgery and applies them to a minimally invasive robot-assisted approach.
Expectant Management
This is the intensive close observation of the patient’s condition without administering any treatment until symptoms appear or change. It is usually used in men with other medical problems and early stage disease.
Radiation therapy
Radiation therapy is used to treat prostate cancer. Radiation therapy is a general term used to describe several types of treatment, including the use of high-powered x-rays, the introduction of radioactive materials into the body, or the injection of substances into the bloodstream.
Different types of radiation therapy:
External beam radiation therapy (EBRT): this is the most common type of radiation therapy. These x-rays destroy tumor cells by damaging their DNA. During treatment, radiation exposure is brief and noninvasive, so patients do not feel discomfort during radiation exposure.
External radiation therapy is usually administered once a day, five days a week. Primary treatment for localized prostate cancer usually requires approximately eight weeks of treatment.
Common side effects of EBRT for prostate cancer include increased urinary frequency; mild burning with urination; weak urinary flow; bowel irritability with mild diarrhea, gas, urgent need to defecate and bowel tenderness; mild irritation of the skin surrounding the rectum; decreased blood cells and fatigue.
Rare complications include significant rectal bleeding, bladder irritability and urethral stricture. Another relatively common remote side effect of radiation is loss of erection, and depends on the use of other treatments such as hormonal treatments and the presence of other diseases that may affect sexual function.
3D Conformal Radiation Therapy
3D conformal radiotherapy is schematically broken down into 3 stages; the acquisition and processing of 3D images, the planning and finally the execution and verification of the treatment. There are limits and uncertainties throughout this process, which uses constantly evolving technologies. The delineation of the target volume and organs at risk, a crucial step in 3D conformal radiotherapy, can vary from one practitioner to another. The safety margins around these volumes, which take into account the internal movements of the organs and the uncertainties of tumor extension, remain empirical and may, once again, be different from one team to another.
There is, however, a consensus among radiation oncologists and medical physicists in recognizing 3D conformal radiotherapy as a more precise and elaborate technique than conventional radiotherapy. The comparison of dosimetric plans showing a decrease in radiation doses to healthy tissues has gained the adherence of the profession.
3D conformal radiotherapy is visibly less toxic at equal doses than conventional radiotherapy.
Intensity Modulated Radiation Therapy
Intensity modulated radiation therapy (IMRT) is a modality that uses computer-controlled X-ray accelerators to deliver precise radiation doses to a malignant tumor to specific areas within the tumor. IMRT allows the radiation dose to conform more precisely to the three-dimensional 3-D shape of the tumor by modulating (controlling) the intensity of the radiation beam.
IMRT makes it possible to focus higher doses to regions within the tumor; while minimizing radiation exposure to surrounding critical normal structures.
IMRT has the potential to reduce treatment toxicity, even with unincreased doses. IMRT does require longer daily treatment times and delivers a lower dose to larger volumes of normal tissue than with conventional radiation therapy.
BRACHYTHERAPY
There are two different approaches to brachytherapy in the treatment of prostate cancer: low dose rate (LDR) and high dose rate (HDR). Prostate brachytherapy is typically delivered using the LDR technique. With LDR brachytherapy, seeds are permanently placed in the prostate. Radiation is administered gradually over a period of months. HDR brachytherapy is performed by placing a highly radioactive source in the prostate temporarily. The radiation treatment is given in a few minutes and is repeated two or three times over the course of several days.
A small percentage of patients will experience urinary obstruction in the weeks following the procedure and will have to use a catheter. These usually disappear within a few weeks and once the edema subsides, the catheter is removed.
Since the radioactive seeds are placed inside the prostate, short-term bowel side effects are uncommon. However, because the anterior part of the rectum is close to the prostate, bowel side effects similar to those of EBRT may occur over time. As with other radiation treatments, erectile sexual dysfunction may occur.
HORMONE THERAPY
Hormone therapy is treatment that eliminates the action of hormones or intercepts their action to stop the growth of prostate cancer. Hormones are chemical substances produced by glands in the body that circulate in the bloodstream. In the case of prostate cancer, male sex hormones can cause the cancer to grow. Drugs, surgery or other hormones can be used to reduce the production of male hormones or prevent them from working.
Hormone therapy used in the treatment of prostate cancer may include the following substances:
– Luteinizing hormone-releasing hormone agonists can prevent the testes from producing testosterone. Examples include leuprolide, goserelin and buserelin.
– Anti-androgens can block the action of androgens (hormones that produce male sex characteristics) such as cyproterone, flutamide, bicalutamide and nilutamide.
– Drugs that can stop the adrenal glands from producing androgens include ketoconazole and aminoglutethimide.
– Orchidectomy is a surgical procedure performed to remove both testicles, the main source of male hormones, to reduce the production of these hormones.
– Estrogens (hormones that produce female sexual characteristics) can prevent the testicles from producing testosterone. However, estrogens are rarely used in the treatment of prostate cancer because of the risk of dangerous side effects.
Men treated with hormone therapy may experience: flushing, impaired sexual function, loss of sexual appetite and bone weakness.
Other treatments
CRYOSURGERY
The treatment uses ultra-fine needles that, by means of sophisticated technology, create ice spheres inside the prostate gland that reach ultra-freezing temperatures of -70ºC, destroying the prostate tissue and the cancer contained inside.
A combination of argon and helium gases allows the temperature to be controlled. The argon gas circulating through the needles generates very low temperatures, causing the formation of ice. The precise creation of ice spheres is used to create a freezing region that exactly matches the size and shape of the prostate. The freezing process is lethal to the cells, killing all prostate tissue.
Prostate cryosurgery treats the entire prostate and aims to freeze the prostate tissue. In this process, the nerves responsible for penile erection can be affected and, as with surgery and radiation therapy, erectile dysfunction is a potential complication of this treatment.
CHEMOTHERAPY
A cancer treatment that uses drugs to interrupt the growth of cancer cells by killing them or preventing them from multiplying. When chemotherapy is given by mouth or injected into a vein or muscle, the drugs enter the bloodstream and can reach cancer cells throughout the body (systemic chemotherapy).
When chemotherapy is placed directly into the spine, an organ, or a body cavity such as the abdomen, the drugs mainly affect cancer cells in those areas (regional chemotherapy).
The way the chemotherapy is given depends on the type and stage of the cancer being treated. Combination chemotherapy is treatment with the use of two or more anticancer drugs.
Biological therapy
Treatment that uses the patient’s immune system to fight cancer. Substances made by the body or in the laboratory are used to boost, direct or restore the body’s natural defenses against cancer. This type of cancer treatment is known as biotherapy or immunotherapy.
High Intensity Focused Ultrasound (HiFu)
A computer-driven medical device designed to treat localized prostate cancer using high-intensity focused ultrasound. The energy is released from an endorectal probe. The ultrasound waves travel through the walls of the rectum without damaging it and are focused on the prostate. This targeting produces an intense and instantaneous heating that causes irreversible destruction of the selected area, without damaging the surrounding tissues.
This therapeutic option is aimed at patients in first intention or as a rescue after failure of radiotherapy.
Dr. Norberto Bernardo is the specialist in charge. To know more about him,